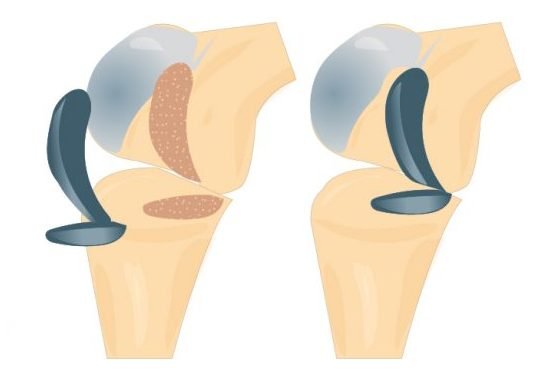
Arthritis leads to the weight bearing surfaces of the knee joint to become wear away. The cartilage layer is damaged and lost and is no longer smooth, leadings to stiffness and pain in the joint. Eventually the joint wears out to such an extent that the bone of the femur grinds on the bone of the tibia as most of the cartilage is lost.
The main indication for a knee replacement is increasing pain that has not been resolved with non-operative measures (pain relief medications, weight loss, physiotherapy etc.) and is markedly affecting one’s quality of life.
Osteoarthritis either develops in just one compartment of the knee, inner (medial) compartment, outer (lateral) compartment or under the knee cap (Patello-femoral compartment), but can involve 2 or all 3 compartments of the knee as well. When only one compartment is involved, a uni-compartmental knee replacement (UKR) is the operation of choice and is designed to replace the worn joint surfaces on one side of the joint, thereby relieving pain and improving function.
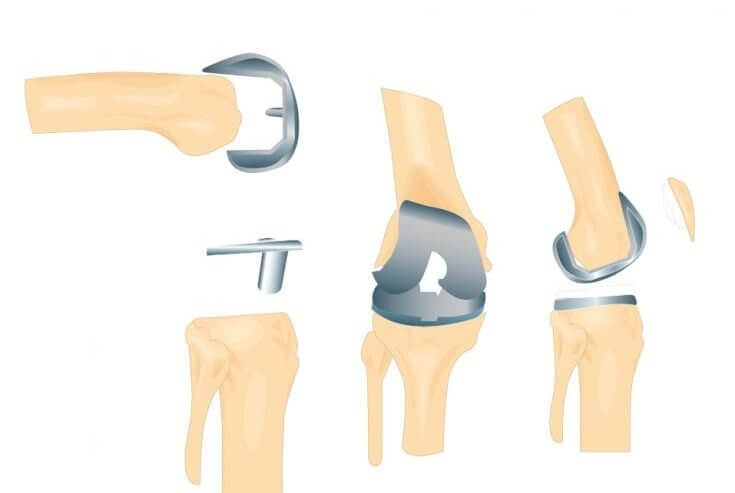
If the arthritis involves more of the knee then a total knee replacement (TKR) may be recommended. This decision may sometimes be made at the time of surgery when the surgeon can directly inspect the joint surfaces. A TKR replaces the surfaces of the knee with metal and plastic in between. Sometimes a single fully plastic tibial component is used.
Surgical technique:
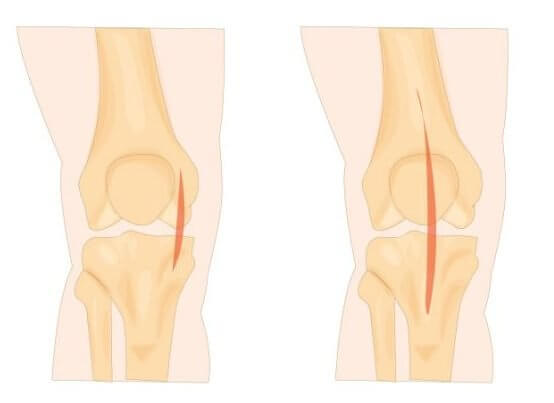
Incisions: There are several different approaches to the knee, depending on the preference of the surgeon– Medial parapatellar, Subvastus and Midvastus. The length of the incision is about 15 to 20 cm.
Entering the knee joint: Shifting the patella to the side and exposing the knee joint
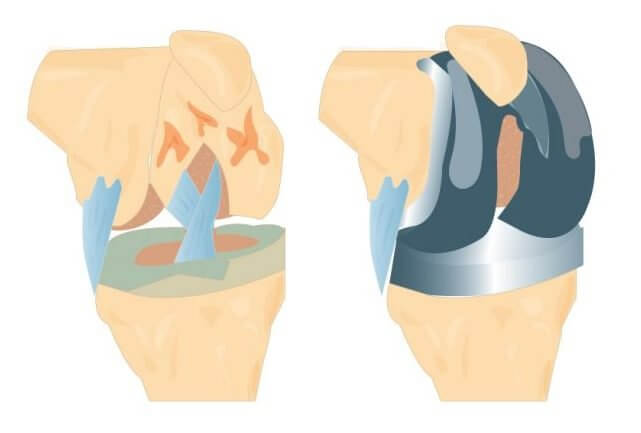
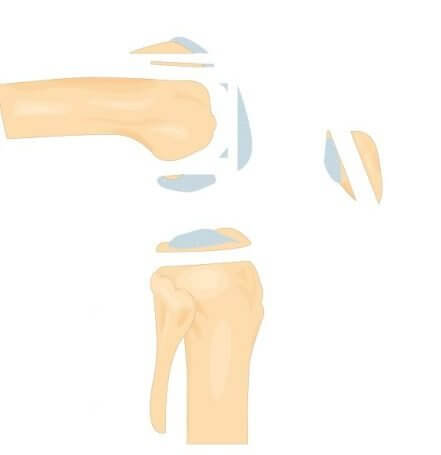
Bone preparation: The damaged cartilage surfaces at the ends of thefemur, tibia and kneecap (patella), are removed along with a small amount of underlying bone. using special Jigs.
1. Ankle Pumping
Lying on your back or sitting up in bed, move your ankles up and down as far as possible while keeping your legs straight.
You may also move your ankles in circles.
This should be performed every hour that you are awake, pumping each ankle 20 times.
*If you keep your knee straight during this exercise you will feel a stretch in your calf muscles.
Position the implants: After determining the appropriate size and shape, the removed cartilage and bone is replaced with metal components that recreate the surface of the joint. These metal parts may be cemented or “press-fit” into the bone.The undersurface of the patella (kneecap) is cut and resurfaced with a plastic button. Some surgeons do not resurface the patella, depending upon the case.
Final inspection: A plastic spacer is inserted between the metal components to create a smooth gliding surface and the knee joint is checked for stability. Closure of incision: special non absorbable sutures for the mechanical layer (capsule or facia), then absorbable stitches for Subcutaneous layer.
Exercises to Prevent Post-Operative Complications:
1. Deep Breathing and Coughing
This exercise can be performed in bed or in any other position (e.g. lying in bed or sitting in chair).
Take five deep breaths followed by two to three coughs every 15 minutes.
This should be performed every hour of the day that you are awake.
2. Ankle Pumping
Lying on your back or sitting up in bed, move your ankles up and down as far as possible while keeping your legs straight.
You may also move your ankles in circles. This should be performed every hour that you are awake, pumping each ankle 20 times.
*If you keep your knee straight during this exercise you will feel a stretch in your calf muscles.